
A 37-Year-Old Woman With Headaches and New-Onset Seizures
HISTORY
 A 37-year-old woman with a 2-year history of migraine headaches presents to the emergency department with a new-onset seizure. Two days earlier the patient had complained of a headache, similar in quality to her previous migraines. One day earlier she experienced blurred vision and a decrease in hearing; these symptoms were atypical of her migraines. On the day of admission, her spouse witnessed seizure-like activity of 10 seconds duration with loss of bladder control. During emergency services transport, the patient had a generalized seizure.
A 37-year-old woman with a 2-year history of migraine headaches presents to the emergency department with a new-onset seizure. Two days earlier the patient had complained of a headache, similar in quality to her previous migraines. One day earlier she experienced blurred vision and a decrease in hearing; these symptoms were atypical of her migraines. On the day of admission, her spouse witnessed seizure-like activity of 10 seconds duration with loss of bladder control. During emergency services transport, the patient had a generalized seizure.
Previous evaluation of her headaches 2 years earlier, including a CT angiogram of her head, was unremarkable. Hypertension was diagnosed when she was in her twenties. She had an uncomplicated pregnancy at age 20 and an uncomplicated cesarean delivery of twin girls 16 days before this admission. Her only medication is a folate supplement.
PHYSICAL EXAMINATION
Temperature is 37.3°C (99.1°F); heart rate, 119 beats/min; blood pressure, 201/107 mm Hg; respiration rate, 15 breaths/min; oxygen saturation, 97% on room air. The patient appears lethargic. Pupils are reactive to light bilaterally. The remainder of the neurologic examination is unremarkable. The neck is supple without cervical rigidity. Heart and lungs are normal. Her abdomen has a healing surgical wound. Extremities and skin are normal.
LABORATORY AND IMAGING RESULTS
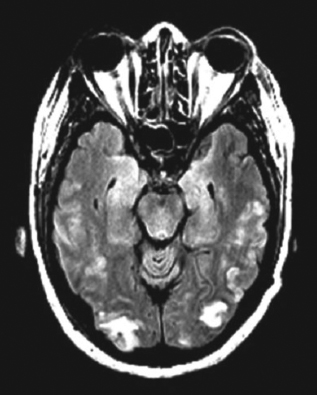
Her white blood cell count is 14,800/μL with a normal differential. Her red blood cell and platelet counts are normal. Serum chemistry, liver function, and coagulation test results are normal. Urinalysis reveals a protein level of higher than 500 mg/dL. A T2-flair image from an MRI scan is shown here.
WHAT'S YOUR DIAGNOSIS?
Answer on next page
ANSWER: LATE POSTPARTUM ECLAMPSIA WITH POSTERIOR REVERSIBLE ENCEPHALOPATHY SYNDROME (PRES)

Most cases of eclampsia occur after 28 weeks gestation and within 48 hours of delivery; however, cases occurring outside this timeframe are well described. Late postpartum eclampsia, as was seen in this patient, has been observed up to 4 weeks postpartum. Any presentation that is somewhat atypical (ie, atypical gestational age or focal neurologic signs) warrants further investigation, including lumbar puncture and radiologic imaging.2,3
PRES: A BRIEF OVERVIEW
PRES is a distinct radiologic pattern of vasogenic edema in the setting of neurotoxicity that is strongly associated with eclampsia. The syndrome is distinguished by its focal, symmetric distribution in watershed areas of the parietal and occipital areas of the brain. Contrary to the name, PRES can affect frontal, brainstem, or cerebellar zones as well. Symptoms associated with PRES include headaches, vision changes, focal neurologic signs, alterations in mental status, and seizures. PRES is not unique to eclampsia and is observed in a number of other conditions (Table). PRES is thought to be fully reversible with management of the underlying disorder.4,5
MANAGEMENT OF ECLAMPSIA
Magnesium sulfate is the mainstay of treatment to prevent recurrent eclamptic convulsions. In head-to-head and collaborative trials, magnesium infusion continued for 24 hours after delivery or the last seizure was more efficacious than phenytoin, nimodipine, or benzodiazepines.6 Elevated systemic blood pressure is managed with antihypertensives. Adequate placental perfusion pressure takes priority over returning patients to normotensive levels. When the onset of preeclamptic symptoms is gradual, preventive therapy includes preemptive treatment of hypertension and prophylactic magnesium.1,2
OUTCOME OF THIS CASE
Given this patient’s hypertension, recent delivery, and proteinuria, eclampsia was strongly considered in the differential and magnesium and antihypertensives were started. The late onset of symptoms (16 days postpartum) warranted radiographic imaging. A 24-hour urine protein collection demonstrated 1107 mg of protein/24 hours (normal: 25 to 75 mg/24 hours), which strongly supported the diagnosis of eclampsia. She had no further seizures.
1. Sibai BM. Diagnosis, prevention, and management of eclampsia. Obstet Gynecol. 2005;105:402-410.
2. Sibai BM, Stella CL. Diagnosis and management of atypical preeclampsia- eclampsia. Am J Obstet Gynecol. 2009;200(5):481.e1-e7.
3. Matthys LA, Coppage KH, Lambers DS, et al. Delayed postpartum pre- eclampsia: an experience of 151 cases. Am J Obstet Gynecol. 2004;190:1464-1466. 4. Bartynski WS. Posterior reversible encephalopathy syndrome, part 1: funda- mental imaging and clinical features. Am J Neuroradiol. 2008;29:1036-1042.
5. Bartynski WS. Posterior reversible encephalopathy syndrome, part 2: con- troversies surrounding pathophysiology of vasogenic edema. Am J Neuroradiol. 2008;29:1043-1049.
6. Euser AG, Cipolla MJ. Magnesium sulfate for the treatment of eclampsia:
a brief review. Stroke. 2009;40:1169-1175.