
Authors:
Syed A. A. Rizvi, PhD, MS, MBA
Hampton University School of Pharmacy, Hampton, Virginia
Elizabeth Mancuso, PA-S
UHI CommunityCare Clinic, Miami, Florida
Zafar Qureshi, MD
UHI CommunityCare Clinic, Miami, Florida
Mohammad N. Manzoor, BS
UHI CommunityCare Clinic, Miami, Florida
Citation:
Rizvi SAA, Mancuso E, Qureshi Z, Manzoor MN. VACTERL association. Consultant. 2019;59(3):95-96.
A girl was born full-term at 38 weeks via induced vacuum-assisted vaginal delivery. Complications during the pregnancy had included suspected bilateral hydronephrosis prenatally. At 36 weeks of gestation, a prenatal ultrasonogram was notable for bilateral hydronephrosis and megaureter.
Physical examination. The patient had good perfusion and pulse, with the skin appearing pink and intact. The neonate was small for her age but was well nourished. The patient appeared to lean to the left side. She had limited neck range of motion. There was a curvature of the spine. There were symmetric reflexes on the knees and ankles bilaterally. Mild leg-length discrepancy was present, but with no limitation of hip, knee, or ankle range of motion. There was no spasticity. The compartments were soft, and lymphadenopathy was not appreciated.
Diagnostic tests. Voiding cystourethrogram was performed on the first day of life, and the findings showed a bladder with irregular contour due to severely dilated ureters indenting bladder. There was no evidence of vesicoureteral reflux (VUR).
Later, renal ultrasonography results showed obstruction of the right kidney with right renal enlargement and delayed clearance in the dilated right renal pelvis. The smaller left kidney yielded decreased perfusion to the upper pole and a dilated left renal pelvis. Physical examination showed 14 ribs bilaterally with dextroscoliosis, and “butterfly vertebra” at T6. A skeletal survey showed multiple vertebral and rib anomalies and shortening of the first metacarpal bilaterally (Figure 1). Pre- and post-void mercaptoacetyltriglycine-3 (MAG-3) diuretic renal scans showed right renal enlargement and left megaureter (Figure 2).
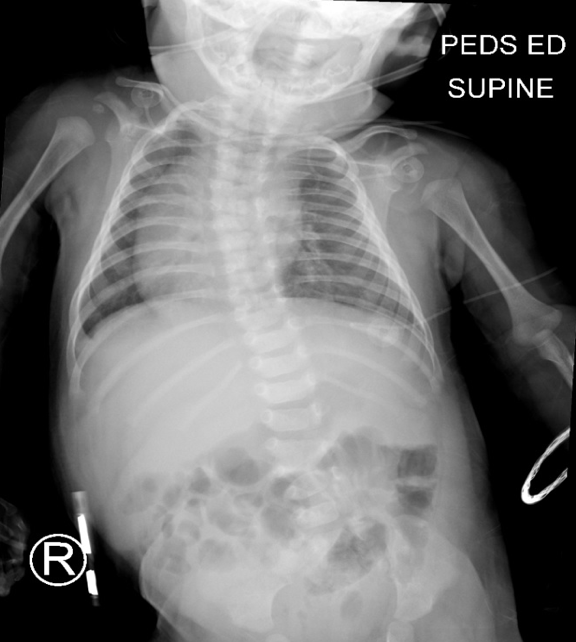
Figure 1. Radiograph showing multiple congenital abnormalities.
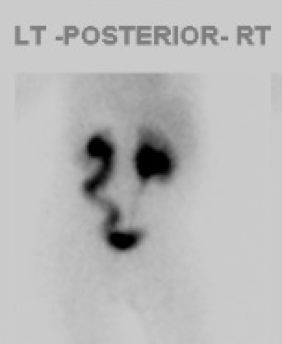

Figure 2. Pre-void (left) and post-void (right) MAG 3 diuretic renal scan showing right renal enlargement and left megaureter.
During the cardiologist visit, a 2/6 systolic ejection murmur at the left lower sternal border and apex was noted. Echocardiography demonstrated dextrocardia, persistent left superior vena cava, patent foramen ovale with left-to-right shunting, and small mid muscular ventricular septal defect with left-to-right shunting. Despite these findings, the patient’s oxygen saturations remained stable; however, these anomalies will eventually require surgical correction.
One month after birth, a cystoscopy with retrograde pyelogram and holmium laser incision of a left ureterocele and right complex dismembered pyeloplasty was performed. Further radiography results showed improvement in the hydronephrosis and absent VUR.
At 8 weeks of age, the patient was taken to a pediatric nephrologist for follow-up regarding congenital hydronephrosis, at which time improvement was noted. At 7 months, the patient had a routine follow-up visit with a urologist. A urine sample yielded positive growth of Pseudomonas, which was treated with ciprofloxacin. The parents were instructed to continue the infant’s prophylactic antibiotic regimen indefinitely.
The initial visit with an orthopedist included assessments for torticollis, congenital scoliosis, hip dysplasia, and pes valgus. Anteroposterior (AP) radiographic view of the pelvis revealed evidence of hip dysplasia with asymmetric femoral ossific nuclei, with less ossification on the left than on the right. AP and lateral radiographs of the spine revealed congenital scoliosis with multiple hemivertebrae noted. A pelvic AP view then noted anatomic alignment of all structures. Mild acetabular dysplasia was noted on the left side. AP and lateral radiographs of the spine showed multiple congenital abnormalities, including mild dextroconvex scoliosis of the thoracic spine and dextroconvex lumbar curve. Multiple segmentation abnormalities were present in the upper thoracic spine, T5-6 and 7, at the T9-10 interspace, and at the L3-4 level. There was marked adenotonsillar enlargement, with narrowing of the nasopharyngeal and oropharyngeal airways.
Repeated spine and pelvic radiographs were recommended after 6 months with no indications for surgery at this time. The orthopedic assessment included VACTERL association.
The patient was seen by a pediatric geneticist, who considered the patient to have features of VACTERL association. A diagnosis of spondylocostal dysostosis (SCD) was ruled out due her cardiac and renal anomalies. The patient’s mother was recommended to have SCD genetic testing completed, especially given the high probability of the mother having another child.
Discussion. VACTERL association is the presence of a minimum of 3 of 7 congenital abnormalities including vertebral, anal, cardiac, tracheoesophageal, renal, and limb abnormalities. The condition was initially described in the 1970s as VATER association, an acronym for vertebral, anal atresia, tracheoesophageal, and renal anomalies. The criteria defining the condition have since been expanded to include vascular, cardiac, and limb abnormalities, hence the acronym VACTERL.1,2 It affects 1 in 10,000 to 40,000 newborns, and a vertebral anomaly is present among 60% to 95% of all persons with VACTERL.3-5
Because co-occurrence of these anomalies is statistically nonrandom, the term association is used rather than syndrome. Most cases of VACTERL association are sporadic, and the exact etiology of this association is unknown and under investigation. Thus, it remains as a diagnosis of exclusion. Due to its multiorgan involvement, VACTERL association is described as a developmental field defect, since malformations during blastogenesis usually result in congenital defects affecting many organ systems. The management of patients with VACTERL association involves long-term care, including surgical corrections of the defects and physical therapy.1,6-8
REFERENCES:
- Solomon BD. VACTERL/VATER association. Orphanet J Rare Dis. 2011;16(6):56.
- Quan L, Smith DW. The VATER association. -Vertebral defects, -Anal atresia, -T-E fistula with esophageal atresia, -Radial and -Renal dysplasia: a spectrum of associated defects. J Pediatr. 1973;82(1):104-107.
- Reutter H, Ludwig M. VATER/VACTERL association: evidence for the role of genetic factors. Mol Syndromol. 2013;4(1-2):16-19.
- Khoury MJ, Cordero JF, Greenberg F, James LM, Erickson JD. A population study of the VACTERL association: evidence for its etiologic heterogeneity. Pediatrics. 1983;71(5):815-820.
- Botto LD, Khoury MJ, Mastroiacovo P, et al. The spectrum of congenital anomalies of the VATER association: an international study. Am J Med Genet. 1997;71(1):8-1
- Martínez-Frías ML, Frías JL, Opitz JM. Errors of morphogenesis and developmental field theory. Am J Med Genet. 1998;76(4):291-29
- Chen Y, Liu Z, Chen J, et al. The genetic landscape and clinical implications of vertebral anomalies in VACTERL association. J Med Genet. 2016;53(7):431-43
- Hersh JH, Angle B, Fox TL, Barth RF, Bendon RW, Gowans G. Developmental field defects: coming together of associations and sequences during blastogenesis. Am J Med Genet. 2002;110(4):320-323.