
Chronic Obstructive Pulmonary Disease: Impact of Symptoms on Activities of Daily Living and Quality of Life
ABSTRACT: The burden of chronic obstructive pulmonary disease (COPD) to patients and society is substantial. As the disease progresses, activities of daily living—from the most basic of tasks to more involved activities—are limited, and quality of life is diminished. Dyspnea, the most burdensome symptom of COPD, worsens over time, reducing exercise tolerance, which further limits daily activities and reduces health status. Due to the progressive nature of COPD, patients may be unaware of the extent of their disability or unable to recognize worsening of symptoms. Therefore, it is important for primary care physicians to evaluate patients for respiratory symptoms and ability to perform activities of daily living and to educate their patients on the disease and associated risk factors. As the first point of contact for most patients with COPD, primary care physicians play a critical role in diagnosing COPD as early as possible and initiating appropriate therapy, thereby alleviating the detrimental clinical consequences of COPD and its symptoms.
__________________________________________________________________________________________________________________________
Chronic obstructive pulmonary disease (COPD) has replaced cerebrovascular diseases as the third-leading cause of death in the United States.1 An estimated 12 million adults have a physician diagnosis of COPD, and 12 million more are estimated to have undiagnosed COPD.2 The clinical and economic burden of the disease is substantial.3 In 2006 alone, there were 672,000 hospitalizations due to COPD in the United States.4 In developed countries, exacerbations of COPD represent the greatest burden on the health care system.3 The National Heart, Lung, and Blood Institute projected the total cost of COPD to be $49.9 billion in the United States in 2010.2,4
The pathophysiology of COPD is not completely understood, but it is characterized by airflow obstruction that is not fully reversible, chronic inflammation, and structural changes in the airways.3 In patients who develop COPD, cigarette smoke or other noxious particles cause an exaggerated inflammatory response that is associated with a specific pattern of increase in inflammatory cell types in different parts of the lung.3 The pathogenesis of COPD is further worsened by an increase in oxidative stress and proteinase activity, which leads to the breakdown of connective tissue such as elastin.3 In the lungs of patients with COPD, the airways lose their elasticity and many of the walls between the alveoli are destroyed, leading to tissue destruction and gas exchange abnormalities characteristic of emphysema.3,5 The airway walls also become thicker and inflamed, and mucus hypersecretion occurs in some patients (Figure 1), clogging the bronchioles and leading to a chronic productive cough characteristic of chronic bronchitis.3,5 These pathological changes are coupled with a gradual worsening of COPD symptoms and disease severity with increasing impact on patients’ daily lives.3

CHARACTERISTIC FEATURES OF COPD AND DISEASE PROGRESSION
The burden of COPD on an individual is dependent on the degree of airflow limitation and the severity of symptoms, including dyspnea, sputum production, wheezing, and chest tightness.3 Acute exacerbation, which is generally defined as an increase in COPD symptoms (eg, dyspnea, cough, and/or sputum) that is beyond the normal day-to-day variation,3 results in greater disease burden for the patient3 and may contribute to more rapid progression of COPD.6-9
Dyspnea is the most common reason patients with COPD seek medical care.3,10 It occurs as a result of lung hyperinflation, which reduces inspiratory capacity and increases functional residual capacity, making it more difficult for patients to move air in and out of the lungs, particularly during exercise.3,11 Hyperinflation, which occurs as a result of air trapping during expiration, can develop early in COPD.3 Early in the disease, patients generally experience dyspnea only during unusual exertion.3 As COPD and airflow limitation progress, patients experience dyspnea with minimal effort; eventually, it is present during everyday activities or even during rest.3
The gradual progressive and chronic nature of the symptoms of COPD may lead to a diminished ability of patients to recognize the effects of COPD on their daily functioning. In a recent survey (“Confronting COPD in America”) of 573 patients with COPD, many of those with substantial functional impairment, determined by scores from the validated Medical Research Council (MRC) dyspnea scale,12 did not recognize their condition as severe.13 In fact, 36% of patients with the most severe grade of dyspnea (score of 5) described their condition as “mild” or “moderate.”13 Similarly, in a telephone survey of 3265 patients with COPD in North America and Europe, 60% and 36% of patients with the second most severe (score of 4) and the most severe (score of 5) grade of dyspnea, respectively, based on the MRC dyspnea scale reported their condition as “mild” or “moderate.”14 This diminished ability of patients to recognize the severity of their condition may lead to a delay in seeking treatment and a greater impact of the disease.
IMPACT OF COPD SYMPTOMS ON ACTIVITIES OF DAILY LIVING AND QUALITY OF LIFE
The importance of recognizing and treating worsening of COPD symptoms is underscored by the negative impact of these symptoms on patients’ basic activities of daily living and quality of life. Most patients included in the “Confronting COPD in America” survey reported that COPD limits what they can do “some or a lot” in normal physical exertion (70%), lifestyle (58%), household chores (56%), social activities (53%), and sleeping (50%).13 Although more than half of the patients surveyed were retired, 51% of patients also reported that COPD limits their ability to work, with 34% reporting that COPD keeps them from working and 17% stating that COPD limits the amount or kind of work they can perform.13
In a telephone survey of patients with COPD in North America and Europe, 36% of respondents reported that their COPD kept them from working, limited their ability to work, or caused them working time loss in the past year.14 In addition, functional limitations in sports and recreation, social activities, household chores, sex life, and family activities due to COPD were reported by a similar or greater percentage of middle-aged patients (aged < 65 years) compared with older patients (aged ≥ 65 years).14 However, limitations in normal physical exertion were reported by significantly fewer middle-aged patients compared with older patients (56% versus 62%, P < .05).14
Evidence suggests that patients particularly are affected by their COPD symptoms during the morning hours. Findings from a quantitative Internet interview of 803 patients with COPD showed that morning was most commonly reported (37%) as the time of day when COPD symptoms were worse than usual.15 When limiting respondents to those with severe COPD, this percentage was even higher (46%).15 In particular, patients’ morning activities that were most affected by COPD included walking up and down stairs, putting on shoes and socks, making the bed, showering and bathing, drying the body with a towel, and dressing.15
Similar findings were observed in a study of 2441 patients with COPD.16 Patients reported that all of their COPD symptoms (breathlessness, phlegm, coughing, wheezing, and chest tightness) were most troublesome upon waking up in the morning.16 The morning activities most affected by COPD symptoms were washing, dressing, drying, and getting out of bed, while the daily activities most affected were going up and down stairs, doing heavy household chores, going shopping, and doing sports or hobbies (Figure 2).16 In addition, 13% of the patients reported that they needed assistance to perform their daily activities, and a majority of those patients believed that they were a burden to others for this reason.16
Dyspnea also showed a strong association with poorer health status in a recent meta-analysis of 66 studies in patients with COPD.17 In that analysis, other COPD symptoms, including sputum production, chronic cough, wheezing, and fatigue, also were associated with poorer health status.17 These findings are particularly important, as health status has been recognized as a major factor affecting patients’ quality of life.18
Taken together, these data suggest that COPD has a substantial negative impact on patients’ daily functioning, from the most minor of daily tasks to more involved activities, and that it results in substantial decrements to patients’ health status. These effects in turn lead to poorer quality of life in patients with COPD.18

EFFECT OF COPD SYMPTOMS ON EXERCISE TOLERANCE
Exertional dyspnea occurs in patients with COPD as a result of dynamic hyperinflation, which involves an increase in air trapping in the lungs during exercise.3 This phenomenon contributes substantially to exercise intolerance in patients with COPD.3,11 Patients with COPD often experience a downward spiral of reduced ability to exercise and physical deconditioning and fatigue, leading to further reduction in exercise tolerance and increasing disability.18,19
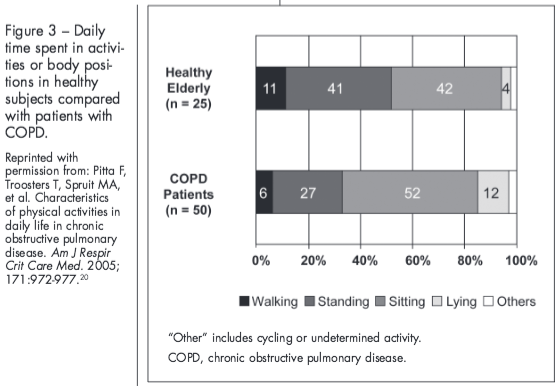
Findings from a study in elderly patients with COPD (n = 50) and healthy elderly subjects (n = 25) showed that patients with COPD are considerably less active than their healthy counterparts.20 They spent a smaller percentage of time during the day walking or standing and a greater percentage of time in the sitting or lying position compared with healthy subjects (Figure 3).20 In addition, patients with COPD experienced significantly (P < .0001) reduced movement intensity (1.8 m/s2) during walking compared with healthy subjects (2.4 m/s2).20 In that study, activity level (walking and standing time) was positively correlated with exercise capacity (based on 6-minute walking distance) in patients with COPD.20
Diminished exercise capacity is a strong indicator of health status impairment3,21 and poorer prognosis.3 In addition, in a study in 452 patients with COPD, increased disability as measured by the Valued Life Activities scale was associated with onset of depression, assessed using the Geriatric Depression Scale Short Form.22 Taken together, these findings highlight the substantial limitations to exercise capacity experienced by patients with COPD and the detrimental clinical consequences of such disability.22
EFFECT OF COPD SEVERITY ON EXERCISE TOLERANCE AND DAILY ACTIVITIES
Exercise tolerance and ability to perform daily activities generally worsen as COPD progresses.3,12,19,23 As COPD severity increases, patients lose muscle bulk and experience diminished exercise endurance.19 This decrement is most noticeable in patients at Global Initiative for Chronic Obstructive Lung Disease (GOLD) stages II (moderate: forced expiratory volume in 1 second [FEV1] % predicted 50% to < 80%), III (severe: FEV1 % predicted 30% to < 50%), and IV (very severe: FEV1 % predicted < 30% or < 50% plus chronic respiratory failure).3 Findings from a study of 100 patients with COPD showed that as patients’ disability (measured using the MRC scale) increases, there is a progressive and significant (P ≤ .003) decline in exercise tolerance (based on shuttle walking distance) and diminished ability to perform daily activities (assessed using the Nottingham Extended Activities of Daily Living scale).12
The effect of COPD disease severity on daily activities and health status was assessed in 2 cross-sectional studies of 1596 patients with moderate COPD and 2012 patients with severe or very severe COPD.23 Patients’ ability to perform activities of daily living (assessed using the London Chest Activity of Daily Living), including self-care, household chores, physical activity, and leisure activity, was significantly (P < .0001) diminished in patients with severe or very severe COPD compared with patients with moderate COPD.23 Approximately two-thirds of patients with severe or very severe COPD versus one-third of patients with moderate COPD reported that their disease affected them “much” in their daily lives.23 In addition, patients with severe or very severe COPD had significantly (P ≤ .0001) worse health status, based on the EuroQol-5D visual analogue scale, than patients with moderate COPD.23 These findings show that the effects of COPD on patients’ ability to perform daily activities and health status worsen with increasing severity of the disease and highlight the need for initiating appropriate COPD therapy as early as possible in the disease process to minimize the negative impact on patients’ daily lives.
ROLE OF PRIMARY CARE PHYSICIANS
As the primary point of contact for many patients with COPD,24 primary care physicians play an important role in COPD prevention, early diagnosis, and appropriate management. Physicians should encourage smoking cessation in patients with or without a diagnosis of COPD, as smoking is a key factor in the development and progression of COPD.3 Educating patients about other inhalational exposures that increase the risk of COPD, including dust and chemicals or air pollution, also is important.3
The GOLD guidelines recommend that a diagnosis of COPD, which is confirmed using spirometry (postbronchodilator FEV1/forced vital capacity [FVC] ratio of < 0.70), should be considered in patients with symptoms of COPD (eg, dyspnea, chronic cough, or sputum production) and/or exposure to risk factors for the disease.3 Recent COPD guidelines issued by the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society recommend against using spirometry for COPD screening in patients who do not have respiratory symptoms.25 However, if patients have symptoms of COPD but do not recognize them, they would fail to meet criteria for spirometry screening,25 which may lead to a delay in diagnosis. Given the substantial burden of the disease and the benefits of early intervention, early screening of COPD using alternative or less expensive tools may be beneficial.
The Lung Function Questionnaire (LFQ) recently was developed as a tool to aid in COPD screening.26 The LFQ is a 5-item self-administered questionnaire, where a total score of ≤ 18 suggests an increased risk of airflow obstruction.26 In a study of 1575 patients aged ≥ 30 years who had a smoking history of 10 pack-years and were not taking asthma or COPD medications, an LFQ score of ≤ 18 identified a prevalence of obstructive lung disease of approximately 18% in a primary care setting; these cases were confirmed by an FEV1/FVC ratio of < 0.70.26 If office spirometry testing is not available, the LFQ is a simple and convenient way for primary care physicians to identify patients who may have COPD and may need a referral for spirometry testing.26
Because patients may fail to recognize the severity of their disease, it is important for primary care physicians to evaluate respiratory symptoms in their patients and explore the impact of dyspnea and other COPD symptoms on their patients’ daily activities and social activities, and work to optimize disease management.3 Patient-physician communication and patient education are critical to this goal because patients’ disease perceptions can affect outcomes,27,28 including quality of life.29 In addition, study findings showed better treatment adherence in patients with compassionate doctors who spend adequate time with them and in patients with greater understanding of their disease and disease management options.30
The Table provides a list of questions that physicians can ask patients to assess their ability to perform activities of daily living and identify disease progression.18 Patients at earlier stages of COPD who experience mild dyspnea on exertion should be able to perform all of the activities listed in the Table, along with additional “productive” activities (employment, gardening, going to movies, recreational travel, social activities, sporting or recreational activities, volunteer work).18 Patients with moderate dyspnea on exertion should be able to perform most of the activities listed as “instrumental” in the Table, while patients with severe COPD may be able to perform only the most basic activities or require assistance completing them.18 Patient responses to these questions can assist in determining the appropriate treatment.3

APPROPRIATE COPD MANAGEMENT
Traditionally, there has been a nihilistic view of COPD management; however, recent guidelines emphasize that this disease is preventable and treatable.3 Currently available COPD treatment options, including pharmacologic and nonpharmacologic therapies, can control and prevent COPD symptoms, reduce exacerbations, and improve exercise tolerance, quality of life, and functional abilities.3,18 Smoking cessation may be the only way to slow the progressive pulmonary function decline in patients with COPD; therefore, primary care physicians should encourage all patients who smoke to quit.3
Conclusions
Symptoms of COPD, including dyspnea, sputum production, wheezing, and chest tightness, negatively affect patients’ ability to perform activities of daily living, which are critical to maintaining quality of life. The chronic and progressive nature of COPD results in gradual decrements to exercise tolerance, health status, and quality of life, which may not always be recognized by the patient. Appropriate COPD management can reduce symptoms and improve patients’ functional abilities, exercise tolerance, and quality of life, underscoring the importance of diagnosing COPD, initiating appropriate treatments, and encouraging smoking cessation as early as possible. As the first point of contact for many patients with COPD, primary care physicians play a critical role in identifying symptoms of COPD in their patients, evaluating patients for disease progression, educating them on their disease and management options, and optimizing treatment.
Acknowledgments
The author thanks Anny Wu, PharmD, and Cynthia Gobbel, PhD, from Scientific Connexions (Newtown, PA) who provided medical writing support funded by AstraZeneca LP (Wilmington, DE).
REFERENCES:
1. Miniño AM, Xu JQ, Kochanek KD. Deaths: preliminary data for 2008. Natl Vital Stat Rep. 2010;59:1-52.
2. National Heart, Lung, and Blood Institute. Morbidity & Mortality: 2009 Chart Book on Cardiovascular, Lung, and Blood Disease. http://www.nhlbi.nih.gov. Accessed September 23, 2011.
3. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. Updated 2010. http://www.goldcopd.org. Accessed September 23, 2011.
4. American Lung Association. Trends in COPD (Chronic Bronchitis and Emphysema): Morbidity and Mortality. Washington, DC: American Lung
Association, Epidemiology and Statistics Unit, Research and Program Services Division; February 2010.
5. National Heart, Lung, and Blood Institute. Diseases and Conditions Index: COPD. Revised June 2010. http://www.nhlbi.nih.gov/health/dci/Diseases/Copd/Copd_WhatIs.html. Accessed
September 23, 2011.
6. Anzueto A. Impact of exacerbations on COPD. Eur Respir Rev. 2010;19:113-118.
7. Rennard SI, Farmer SG. Exacerbations and progression of disease in asthma and chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2004;1:88-92.
8. Tanabe N, Muro S, Hirai T, et al. Impact of exacerbations on emphysema progression in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2011;183:1653-1659.
9. Donaldson GC, Seemungal TAR, Bhowmik A, Wedzicha JA. Relationship between exacerbation frequency and lung function decline in chronic
obstructive pulmonary disease. Thorax. 2002;57:847-852.
10. Kumar S, Gross NJ. The global initiative for COPD: what you need to know. J Respir Dis. 2002;23:549-556.
11. O’Donnell DE, Revill SM, Webb KA. Dynamic hyperinflation and exercise intolerance in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;164:770-777.
12. Bestall JC, Paul EA, Garrod R, et al. Usefulness of the Medical Research Council (MRC) dyspnea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54:581-586.
13. Confronting COPD in America: Executive Summary. http://www.aarc.org. Accessed September 23, 2011.
14. Rennard SI, Decramer M, Calverley PMA, et al. Impact of COPD in North America and Europe in 2000: subjects’ perspectives of Confronting COPD International Survey. Eur Respir J. 2002;20:799-805.
15. Partridge MR, Karlsson N, Small IR. Patient insights into the impact of COPD on morning symptoms, activities and daily life. Curr Med Res Opin. 2009;25:2043-2048.
16. Kessler R, Partridge MR, Miravitlles M, et al. Symptom variability in patients with severe COPD: a pan-European cross-sectional study. Eur Respir J. 2011;37:264-272.
17. Tsiligianni I, Kocks J, Tzanakis N, et al. Factors that influence disease-specific quality of life or health status in patients with COPD: a review and meta-analysis of Pearson correlations. Prim Care Respir J. 2011;20:257-268.
18. Belfer MH, Reardon JZ. Improving exercise tolerance and quality of life in patients with chronic obstructive pulmonary disease. J Am Osteopath Assoc. 2009;109:268-278.
19. Sin DD, Man SFP. Skeletal muscle weakness, reduced exercise tolerance, and COPD: is systemic inflammation the missing link? Thorax. 2006;61:1-3.
20. Pitta F, Troosters T, Spruit MA, et al. Characteristics of physical activities in daily life in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171:972-977.
21. Jones PW. Health status measurement in chronic obstructive pulmonary disease. Thorax. 2001;56:880-887.
22. Katz PP, Julian LJ, Omachi TA, et al. The impact of disability on depression among individuals with COPD. Chest. 2010;137:838-845.
23. Rodriguez Gonzalez-Moro JM. Impact of COPD severity on physical disability and daily living activities: EDIP-EPOC I and EDIP-EPOC II studies. Int J Clin Pract. 2009;63:742-750.
24. Barr RG, Celli BR, Martinez FJ, et al. Physician and patient perceptions in COPD: the COPD Resource Network Needs Assessment Survey. Am J Med. 2005;118:1415.e9-1415.e17.
25. Qaseem A, Wilt TJ, Weinberger SE, et al. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of
Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Ann Intern Med. 2011;155:179-191.
26. Mintz ML, Yawn BL, Mannino DM, et al. Prevalence of airway obstruction assessed by Lung Function Questionnaire. Mayo Clin Proc. 2011;86:
375-381.
27. Kaptein AA, Scharloo M, Fischer M, et al. Illness perceptions and COPD: an emerging field for COPD patient management. J Asthma. 2008;45:
625-629.
28. Scharloo M, Katpetin A, Weinman JA, Willems LNA, Roojimans HGM. Physical and psychologic correlates of function in patients with chronic obstructive pulmonary disease. J Asthma. 2009;37:17-19.
29. Scharloo M, Kaptein AA, Schlösser M, et al. Illness perceptions and quality of life in patients with chronic obstructive pulmonary disease. J Asthma. 2007;44:575-581.
30. George J, Kong DCM, Thoman R, Stewart K. Factors associated with medication nonadherence in patients with COPD. Chest. 2005;128:3198-3204.