
Authors:
Scott Friedman, DO; Jorge Suening, MD; and Morgan Minelli
Citation:
Friedman S, Suening J, Minelli M. Extracardiac rhabdomyoma and spindle-cell lipoma of the upper back. Consultant. 2018;58(5):e164.
A 55-year-old white man with no significant medical history presented to a dermatology office for assessment of a soft lump on his left upper back. He had noticed the lump approximately 15 years ago; it had enlarged slowly over the first few years and had increased rapidly in size over the past year.
History. There were no modifying factors or any history suggesting trauma, infection, or malignancy in the affected area. He was asymptomatic aside from the noticeable protruding mass. He denied symptoms of fatigue, weight changes, and pain or discomfort in the area. The man’s family history was positive for melanoma, but he had no history of soft-tissue tumors.
Physical examination. The patient’s height was 185 cm and his weight was 86.2 kg, corresponding to a body mass index (BMI) of 25 kg/m2. A compressible, nontender, fluctuant, freely mobile, subcutaneous mass measuring 8.0 × 6.0 cm was located on his left upper back. There were no noticeable discolorations, indurations, or other palpable masses. He had full range of motion, strength within normal limits, and intact reflexes of his upper extremities bilaterally.
Diagnostic tests. Based on the texture and location of the mass, the initial clinical impression was that of a subcutaneous cyst rather than a lipoma. However, sliding the fingers off the edge of the mass elicited a positive slipping sign, which suggested lipoma.1 Needle aspiration of the mass, performed to evaluate composition, initially did not yield fluid. However, the area bled profusely with frank blood, and a concern for vascularity and malignancy prompted further workup.
Ultrasonography findings showed an elongated, slightly echogenic mass with discrete borders within the subcutaneous soft tissues, with a similar appearance to the surrounding fat, likely representing a lipoma. There was no internal color Doppler flow to suggest vascularity and no presence of fluid collection.
Treatment. A 4.0-cm linear incision was made under local anesthesia on the left upper back at the T6-7 vertebral level, between the left scapular line and the posterior median line (Figure 1). Careful dissection revealed several soft, irregularly shaped to lobulated, dark red to heme-colored masses resembling muscle tissue, henceforth referred to as specimen A. Further exploration revealed a lobulated, fluctuant, and well-encapsulated light-yellow mass, henceforth referred to as specimen B, which was excised en masse (Figure 2).

Figure 1: Local excision of the mass was accomplished via a 4.0-cm linear cutaneous incision through the deep dermal tissue in the upper left back, just below the inferior border of the scapula at the T6-7 vertebral level.

Figure 2: A 16.5 × 8.2 × 4.3-cm fluctuant, lobulated, encapsulated, and compressible red to yellow voluminous adult extracardiac rhabdomyoma (left) was excised. Several soft, lobulated to irregularly shaped, dark red to heme-colored SCLs resembling muscle tissue (top right) also were excised, with the largest measuring 3.6 × 3.4 × 3.0 cm.
Diagnosis. Dermatopathology test results showed specimen A to be skeletal muscle that showed striations and nuclei toward the periphery of the cells along with focal amounts of subcutaneous fat. The dermatopathology report noted that the differential diagnosis included “normal skeletal muscle for the anatomic area, and in the right clinical context, rhabdomyoma.” Immunohistochemical staining tests of specimen A were negative for S-100 protein and positive for actin, desmin, and myoglobin, suggesting a rhabdomyoma as opposed to normal skeletal muscle.2
Dermatopathology test results showed specimen B to be a lipoma with focal features of a spindle-cell lipoma (SCL). According to the dermatopathology report, “Histological sections demonstrate well-circumscribed lobules of subcutaneous fat that are relatively normal in size and appearance, with some areas showing an increase in normal bundles of collagen and bland spindle cells.” Immunohistochemical staining test results of specimen B were positive for CD34, suggesting SCL.3 With a diameter greater than 10 cm, specimen B met the criteria for a giant lipoma.4,5
Outcome of the case. Follow-up visits at 2, 4, and 8 weeks showed a decrease in the size of the lump on the patient’s back, with no muscle weakness or other physical limitations. Although referral is not routinely required, the possibility for malignant transformation of giant lipomas and rhabdomyomas prompted referral of the patient to an oncologist for comprehensive evaluation, irrespective of the benign nature of the tumors.5-7
DISCUSSION
Rhabdomyomas are rare and often benign mesenchymal soft-tissue tumors that derive from striated cardiac or skeletal muscle.8 They can be distinguished as cardiac or extracardiac forms.7 Extracardiac rhabdomyomas are further categorized into adult, fetal, or genital subtypes.9
Cardiac rhabdomyomas occur more often in the pediatric population, particularly from birth to 3 years of age, and among individuals with tuberous sclerosis, a multisystem genetic disorder manifested by cardiac rhabdomyomas, hypopigmented ash leaf macules, shagreen patches, and seizures.10,11
Adult extracardiac rhabdomyomas are more commonly found in men aged 40 to 60 years.2 Patients with an adult extracardiac rhabdomyoma commonly present with a mass in the head and neck region.2,7 Although rhabdomyomas rarely metastasize, their growth in the oral mucosa or pharynx may compress surrounding neurovascular structures, causing hoarseness, dysphagia, and reduced perfusion that can lead to tissue ischemia and necrosis.2,12 Rarely, adult extracardiac rhabdomyomas present on the back and extremities.10
Genital extracardiac rhabdomyomas are most often found among women aged 40 to 60 years who present with dyspareunia.9
In contrast, rhabdomyosarcomas are highly malignant mesenchymal tumors characterized by muscle differentiation and a predilection for the genitourinary tract, the head and neck region, and the extremities. They more commonly occur in the pediatric population.
Lipomas are the most common benign tumors of mesenchymal origin and are composed of mature adipocytes encapsulated within a fibrous capsule.1 They present in men and women aged 40 to 60 years and have a prevalence of 2.1 per 1000 individuals.1 SCLs occur more frequently in men aged 40 to 70 years.3 Lipomas occur as solitary or multiple masses with a predilection for the posterior neck, shoulder, back, trunk, and extremities. Clinically, they present as a fluctuant, compressible, and nontender subcutaneous mass.1 A positive slipping sign helps differentiate lipomas from cysts. Lipomas grow very slowly and reach an average size of 2 cm.1 Any lipoma greater than 5 cm on the upper extremity or greater than 10 cm on the trunk or back and with a mass greater than 1000 g is classified as a giant lipoma and should be resected to rule out malignant potential.4,13 SCL is a rare subtype of a lipoma14 that easily can be mistaken for a liposarcoma.6 SCLs commonly grow to 2.5 cm and frequently are located on the posterior neck and upper back.3,14 The diagnosis of lipomas is clinical, and no imaging studies are required. Asymptomatic lipomas require no treatment but often are removed for cosmetic reasons.1
Immunohistochemically, rhabdomyomas stain positive for the myogenic markers desmin, actin, and myoglobin.2,3 They stain negative for S-100 protein, a tumor marker for which melanomas stain positive (Figure 3). Microscopic features of rhabdomyomas include polygonal cells arranged in solid sheets, cross-striations elucidated by phosphotungstic acid–hematoxylin staining, peripherally located nuclei, absent mitotic features, and deeply eosinophilic cytoplasm that may be granular or vacuolated due to glycogen.2 By comparison, rhabdomyosarcomas present with rhabdomyoblasts and stain positive for desmin.7
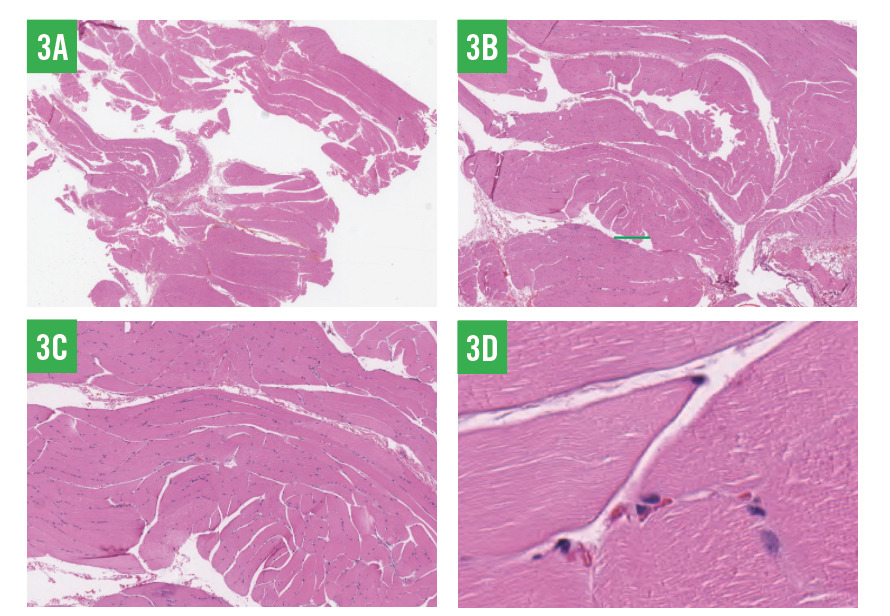
Figure 3: Skeletal muscle cells showing few cross-striations, peripherally located nuclei, abundant eosinophilic cytoplasm, and focal amounts of subcutaneous fat; necrosis or mitotic activity was not noted. The specimen was negative for S-100 protein and positive for actin, desmin, and myoglobin, all of which supported the diagnosis of adult extracardiac rhabdomyoma (3A, ×0.5; 3B, ×2; 3C, ×5; 3D, ×20).
Microscopic features of SCLs include mature adipocytes interspersed between ropey collagen bundles and bland spindled cells arranged uniformly with narrow bipolar cytoplasmic processes (Figure 4).3 SCLs stain positive for CD34 and stain negative for S-100 protein and desmin.3 S-100 protein may stain positive within mature adipocytes but negative within focal spindle-cell areas.14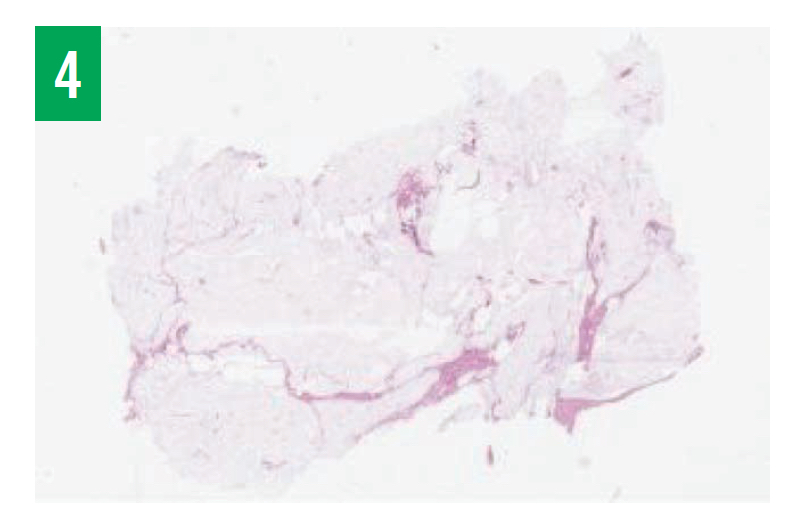
Figure 4: Well-circumscribed lobules of subcutaneous fat that are relatively normal in size and appearance, with some areas showing an increase in normal bundles of collagen and bland spindle cells, supporting the diagnosis of SCL.
Environmental and inherited factors contribute to the development of soft-tissue tumors such as lipomas and rhabdomyomas. Studies suggest a correlation between HMGA2, obesity, and the presence of mesenchymal soft-tissue tumors such as adult extracardiac rhabdomyomas.15 However, our patient was relatively physically healthy, with a BMI of 25 kg/m2 and with cholesterol levels that were within normal limits. The presence of HMGA2 in this patient has yet to be determined. Another study identified the presence of a reciprocal translocation between chromosomes 15 and 17 as the sole abnormality in adult extracardiac rhabdomyoma.12 On the other hand, cardiac rhabdomyomas are typically associated with tuberous sclerosis, a genetic condition caused by an autosomal dominant mutation in TSC1 and TSC2.11
While the cause of rhabdomyoma and lipoma remain uncertain, there are possible mechanisms for the concurrence of the 2 conditions. Since rhabdomyomas and lipomas both originate from mesenchyme—a type of embryonic tissue characterized by loosely associated cells lacking polarity—it can be ascertained that both tumors develop consecutively prior to differentiation.16 Myogenesis is a specific function of mesenchyme; mesenchymal-to-epithelial transition may be the basis for metastasizing cancers such as squamous cell carcinoma. Mesenchymal cells grown in tissue culture tend to form spindle-like shapes and are able to migrate along the extracellular matrix by extending their filopodia through the loose matrix to move in response to various chemotactic molecules.15,17 Morphologically, mesenchymal cells migrate through the extracellular matrix with ease compared with epithelial cells.16,17 Because of this innate ability, mesenchymal cells have the predisposition to differentiate into lipomas, rhabdomyomas, and even metastatic soft-tissue tumors such as rhabdomyosarcomas.15,17
While malignant transformation of rhabdomyoma and lipoma is rare, and local excision is curative, annual physical examinations are recommended to evaluate for reoccurrence.
CONCLUSION
This patient’s case highlights the importance of clinical cutaneous physical examination and dermatopathology tests in the evaluation of patients with subcutaneous masses. To our knowledge, this is the first case of concurrent adult-type extracardiac rhabdomyoma with concurrent giant spindle-cell lipoma on the upper back. Further research is warranted to delineate the cellular mechanisms governing the pathogenesis of these 2 tumors.
Scott Friedman, DO, is a dermatologist at the Cosmetic Dermatology and Vein Center in Lake Orion, Michigan, and the dermatology clerkship professor for the Ross University School of Medicine in Roseau, Commonwealth of Dominica.
Jorge Suening, MD, is a recent graduate of Ross University School of Medicine in Roseau, Commonwealth of Dominica.
Morgan Minelli is a student at Northwestern University in Evanston, Illinois.