
 A 15-year-old girl was referred to a pediatric endocrinologist for evaluation of hyperthyroidism. Her primary concerns were intermittent increases in heart rate and appetite (with a weight gain of 7 kg within the past year), feeling hot at night even in winter, persistent lower extremity edema that had been present since age 4 years, and difficulty in concentrating. She denied having diarrhea, sweating, fatigue, breathing difficulties, hair loss, or changes in hair texture. Recent laboratory test results showed a thyroid-stimulating hormone (TSH) level of 0.02 μIU/mL (normal, 0.1 to 5 μIU/mL) and a free thyroxine level of 2.34 ng/dL (normal, 0.71 to 1.85 ng/dL).
A 15-year-old girl was referred to a pediatric endocrinologist for evaluation of hyperthyroidism. Her primary concerns were intermittent increases in heart rate and appetite (with a weight gain of 7 kg within the past year), feeling hot at night even in winter, persistent lower extremity edema that had been present since age 4 years, and difficulty in concentrating. She denied having diarrhea, sweating, fatigue, breathing difficulties, hair loss, or changes in hair texture. Recent laboratory test results showed a thyroid-stimulating hormone (TSH) level of 0.02 μIU/mL (normal, 0.1 to 5 μIU/mL) and a free thyroxine level of 2.34 ng/dL (normal, 0.71 to 1.85 ng/dL).
 Physical examination showed bilateral exophthalmos (but no lid lag or lid retraction); hyperthyroid stare; a large symmetrical palpable goiter, without thyroid bruits (A); tachycardia, without murmur; and bilateral lower extremity edema consistent with pretibial myxedema (B).
Physical examination showed bilateral exophthalmos (but no lid lag or lid retraction); hyperthyroid stare; a large symmetrical palpable goiter, without thyroid bruits (A); tachycardia, without murmur; and bilateral lower extremity edema consistent with pretibial myxedema (B).
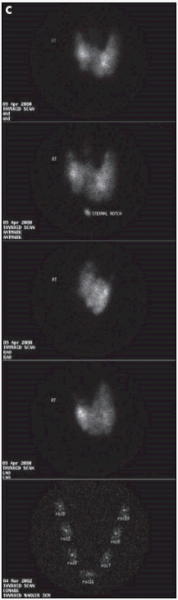
Additional laboratory tests showed that her thyroid-stimulating immunoglobulin levels were within normal limits; however, her thyroid peroxidase antibody level was 38.3 IU/mL (normal, 0 to 10.1 IU/mL), and her antithyroglobulin antibody level was 47.4 IU/mL (normal, 0 to 28.7 IU/mL). Radioactive iodine(Drug information on iodine) (123I) thyroid uptake was elevated at 6 and 24 hours, with values of 57% and 69%, respectively; and a thyroid scintography scan showed homogeneous tracer uptake consistent with Graves disease (C).
 Graves disease is rarer in children (prevalence, 0.02%) than it is in adults (prevalence, 0.40%); the peak incidence of pediatric Graves disease occurs in children aged 11 to 15 years.1 There is a 5:1 female to male preponderance.1 Graves disease is characterized by a diffuse goiter, thyrotoxicosis, associated infiltrative ophthalmopathy, and sometimes infiltrative dermopathy. Weight loss and palpitations are other common findings; however, some patients gain weight. Infiltrative dermopathy is the least common manifestation of the disease, occurring in fewer than 5% of patients. Infiltrative dermopathy, also known as pretibial myxedema, is more commonly seen in patients with hypothyroidism or Hashimoto thyroiditis, or following iodine 131(131I) treatment for thyrotoxicosis. This patient's presentation, which included both weight gain and long-standing infiltrative dermopathy, was thus quite unusual.
Graves disease is rarer in children (prevalence, 0.02%) than it is in adults (prevalence, 0.40%); the peak incidence of pediatric Graves disease occurs in children aged 11 to 15 years.1 There is a 5:1 female to male preponderance.1 Graves disease is characterized by a diffuse goiter, thyrotoxicosis, associated infiltrative ophthalmopathy, and sometimes infiltrative dermopathy. Weight loss and palpitations are other common findings; however, some patients gain weight. Infiltrative dermopathy is the least common manifestation of the disease, occurring in fewer than 5% of patients. Infiltrative dermopathy, also known as pretibial myxedema, is more commonly seen in patients with hypothyroidism or Hashimoto thyroiditis, or following iodine 131(131I) treatment for thyrotoxicosis. This patient's presentation, which included both weight gain and long-standing infiltrative dermopathy, was thus quite unusual.
She underwent ablation of her thyroid with 131I and had a good response. At follow-up 6 weeks later, she did not report palpitations or any symptoms of hypothyroidism. Her facies were improved, with persistent but diminished exophthalmos and hyperthyroid stare and a still-palpable but smaller goiter. However, she still had edema of her lower extremities.
Infiltrative dermopathy does not necessarily resolve with correction of the underlying hyperthyroidism. Options for treatment of Graves dermopathy include high-dose topical corticosteroids, intralesional corticosteroids, and intravenous immunoglobulin. Plasmapheresis and surgical therapies have also been tried. Newer therapies include octreotide, a somatostatin analogue, which is thought to suppress insulinlike growth factor 1, and pentoxifylline, which has demonstrated a decrease in glycosaminogly can production by fibroblasts in vitro.2 High-potency topical glucocorticoids used with an occlusive dressing may cause regression or resolution of the lesion.3,4 Patients with pretibial myxedema may have good outcomes with one of the above therapies.