
How Would You Diagnose These Papules?
History
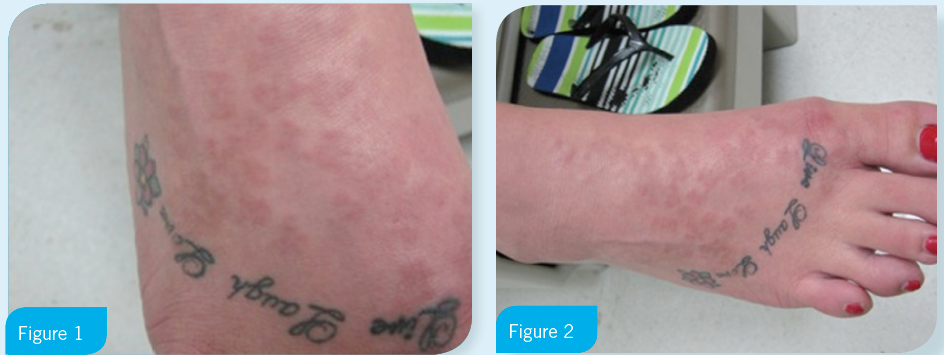
A 23-year-old otherwise healthy female presented with a collection of slightly raised 5 mm to 10 mm salmon-colored papules on the dorsum of both feet (Figures 1 and 2). Since first noticing the papules 3 months ago, they had increased both in size and number.
The patient denied any pain or itching. She had no identifiable cause or trigger. She had used over-the-counter topical steroids for treatment with no improvement. A punch biopsy was performed and showed a “region of histiocytes surrounding a focus of dermis with increased mucin deposition.”
(Answer, podcast and discussion on next page)
Answer: Granuloma annulare
Discussion
Granuloma annulare (GA) presents localized to the dorsum of the hands and/or feet in 75% of cases.1,2 The lesions of localized GA appear as clusters of papules that can vary in color from natural skin tone to erythematous.1 This localized form is most commonly seen in women under 302,3 and is typically asymptomatic with a variable duration.1 The disease is typically self-limited, resolving within 2 years in 50% of cases, and the asymptomatic lesions do not require treatment except for cosmetic reasons.1,2 If treatment is desired for cosmesis, intralesional triacinolone acetonide may be used.2 Alternatively GA can present as disseminated, generalized, perforating, and subcutaneous.4
Although biopsy is not always necessary, histologically these lesions may show feature collagen degeneration, mucin deposition, and infiltration by histocytites.1,2 The presentation of histocytes is variable in GA from pallisading to interstitial.1
Differential Diagnosis
Lichens planus is a disease that is characterized by the six p’s: planar, pruritic, purple, polygonal, papules, and plaques. Lichens planus tends to affect the wrists, forearms, and legs.5 Although primary eruptions of lichens planus typically resolve within 2 years, nearly 50% of patients will have recurrent disease.2,5 Histologically, linear deposits of fibrin and fibrinogen are present within the basement membrane.2
Dermatitis herpetiformis is a severely pruritic rash associated with gluten-sensative enteropathy.2 The rash of dermatitis herpetiformis may be generalized or concentrated on the knees, buttocks, elbows, shoulders, nuchal area, and scalp.2 Histologically, these lesions show microabscesses within the dermal papilla, subdermal vesicles, and neutrophillic and eospinophillic infiltration.2,6
Necrobiosis lipoidica is associated with diabetes with over 50% of patients being insulin dependent.2 Typically presenting on the anterior surface of the legs, the lesion initial presents as a violacious plaque which gradually expands.2 As the lesion expands, the central aspect changes to a waxy yellow and then to an atrophied state.2 The final stages of this lesion are a fibrosis and ulceration. Although a biopsy is not always necessary for diagnosis, histologically, this lesion features pallisading necrobiotic granuloma.7
References:
- Thornsburry L, English J. Etiology, diagnosis, and therapeutic management of granuloma annulare: an update. Am J Clin Dermatology. 2013;14(4):279-290.
- Habif T. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 4th Edition. Mosby; 2003.
- Cyr P. Diagnosis and management of granuloma annulare. Am Fam Physician. 2006;74(10):1729-1734.
- Pătraşcu V, Giurcă C, Ciurea RN, Georgescu CV. Disseminated granuloma annulare: study on eight cases. Rom J Morphol Embryol. 2013;54(2):327-331.
- Usatine R, Tinitigan M. Diagnosis and treatment of lichen planus. Am Fam Physician. 2011;84(1):53-60.
- Bickle K, Roark T, Hsu S. Autoimmune bullous dermatoses: a review. Am Fam Physician. 2002;65(9):1861-1871.
- Dissemond J. Necrobiosis lipoidica diabeticorum. N Engl J Med. 2012;366(26):2502.