 For 2 weeks this past March—2 months after the strongest earthquake to hit Haiti in more than 200 years had struck—I served as part of a physical medicine rehabilitation group sent by Team Canada Healing Hands (TCHH) (Box). The team worked in both Jacmel, a major city on the south coast of Haiti, and in Port-au-Prince. Portau-Prince, Jacmel, and the 80 km of mountainous land between these 2 cities suffered severe damage during the January earthquake.
For 2 weeks this past March—2 months after the strongest earthquake to hit Haiti in more than 200 years had struck—I served as part of a physical medicine rehabilitation group sent by Team Canada Healing Hands (TCHH) (Box). The team worked in both Jacmel, a major city on the south coast of Haiti, and in Port-au-Prince. Portau-Prince, Jacmel, and the 80 km of mountainous land between these 2 cities suffered severe damage during the January earthquake.
My role was to provide medical support for the rehabilitation patients and otherwise support local pediatric services. As things turned out, more than 90% of my time was spent supporting local pediatric services. For the first 10 days, I was the pediatrician for the outpatient department at St Michel, a Jacmel hospital that partially survived the earthquake, and for the last 2 days, I served as pediatrician for the inpatients in the Project Medishare tent in Port-au-Prince.
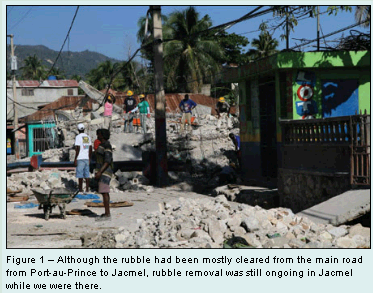
When I arrived, the devastation wrought by the earthquake was immediately evident. Although just about all the rubble (Figure 1) had been cleared from the road that connects the capital to Jacmel (a 2-story–high boulder remained, blocking 1 lane near the top of the pass), there were wide cracks and upheavals in the paved road. The trip from Port-au-Prince to Jacmel took 3 or 4 hours, depending on the time of day and the weather. Almost everything but disaster and disease moves slowly in Haiti.
JACMEL: LONG LINES OF PATIENTS WAITING FOR CARE
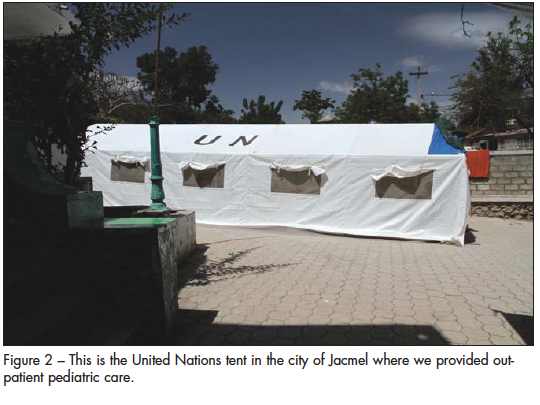
During my time in Jacmel, there was usually a Haitian physician in the St Michel emergency room (ER) and a foreign disaster-relief physician in the outpatient area. In addition, Médecins Sans Frontières (MSF) ran an inpatient service in tents on the site. When I arrived, I took over the pediatric outpatient care, which we provided in a United Nations tent next to the ER (Figure 2).
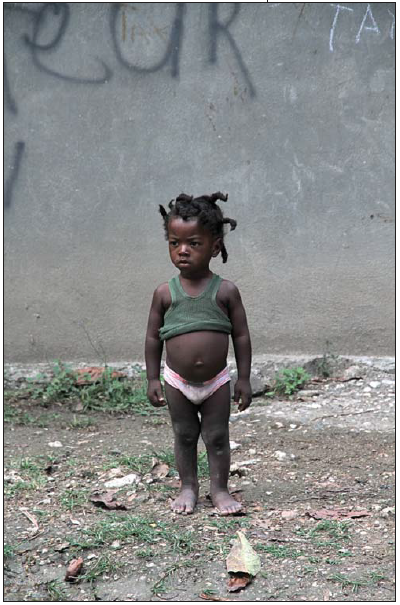
 Families and individuals in the Jacmel area who desired medical care turned up at the St Michel site soon after dawn each day and waited patiently to be seen by a physician. Some waited the entire day. Every morning by the time we arrived, there were several hundred people waiting to be assessed; about one-third were children (Figure 3). At first I was rusty and inefficient, and we did not manage to see all the children the same day they arrived. We gave out numbers to those we did not get to so that they would be seen first the next day. Within a few days, however, my history questions had become more focused, my notes had gotten much shorter, and we managed to see all the children who came to us.
Families and individuals in the Jacmel area who desired medical care turned up at the St Michel site soon after dawn each day and waited patiently to be seen by a physician. Some waited the entire day. Every morning by the time we arrived, there were several hundred people waiting to be assessed; about one-third were children (Figure 3). At first I was rusty and inefficient, and we did not manage to see all the children the same day they arrived. We gave out numbers to those we did not get to so that they would be seen first the next day. Within a few days, however, my history questions had become more focused, my notes had gotten much shorter, and we managed to see all the children who came to us.
Good Creole interpreter a real blessing. I always had an interpreter. Unfortunately, the local Creole interpreters varied considerably in their talent and motivation; when working with them, I was never really comfortable that my questions were understood or that my treatment instructions were adequately translated. However, for the last half of my stay, a first-year Canadian medical student who was fluent in Creole worked with me. After 2 days of listening to my routine instructions for hydration, fever, impetigo, and other common problems, we were able to set up a second examination table on an old desk. Instead of my performing a complete physical exam on every child, the medical student started to assess the less sick-looking children, and I performed a focused examination of each child before he or she left. In addition to providing valuable help with physical exams, the Canadian medical student had brought a portable printer. I designed a form on which to record patient history, exam results, diagnosis, and treatment. Using these forms made a big difference in the thoroughness and efficiency of our assessment and documentation.
Laboratory and diagnostic imaging services were not available unless a family could pay for them—which no one could. In the case of x-rays, this was a moot point; the first week I was there, no film was available, and in the second week, the limited film we had was reserved for inpatients. A laboratory was available for the MSF inpatients but not for outpatients.
 Scrounging for medications. I had brought a duffle bag full of medications—mostly antibiotics—but we used them up quickly. After these were gone, I became good at scrounging for medicine and supplies. There were cupboards with medications in the ER and adult outpatient area, and after the security and health care staff came to know me, I was allowed to take whatever supplies I could find. It was rare to have a first-line drug available, pediatric and liquid formulations were very hard to come by, and some of the bottles had 2009 expiration dates; however, I was happy for anything that might work or that could be made to work. One evening, we met a pharmacist from an American Catholic Church clinic outside Jacmel; he offered to donate supplies, and this allowed me to stock up on liquid acetaminophen, oral rehydration solution, and a topical antifungal.
Scrounging for medications. I had brought a duffle bag full of medications—mostly antibiotics—but we used them up quickly. After these were gone, I became good at scrounging for medicine and supplies. There were cupboards with medications in the ER and adult outpatient area, and after the security and health care staff came to know me, I was allowed to take whatever supplies I could find. It was rare to have a first-line drug available, pediatric and liquid formulations were very hard to come by, and some of the bottles had 2009 expiration dates; however, I was happy for anything that might work or that could be made to work. One evening, we met a pharmacist from an American Catholic Church clinic outside Jacmel; he offered to donate supplies, and this allowed me to stock up on liquid acetaminophen, oral rehydration solution, and a topical antifungal.
When necessary, we made suspensions by pulverizing tablets and mixing the powder in bottled water. I found a supply of 100-mL bottles of sterile normal saline; we emptied out the saline and used the containers for our formulations. We put duct tape on the bottles and wrote how much of the medication to take and how often to take it. We gave out 10-mL syringes and used duct tape to mark the level of the desired volume to help mothers give the correct dose.
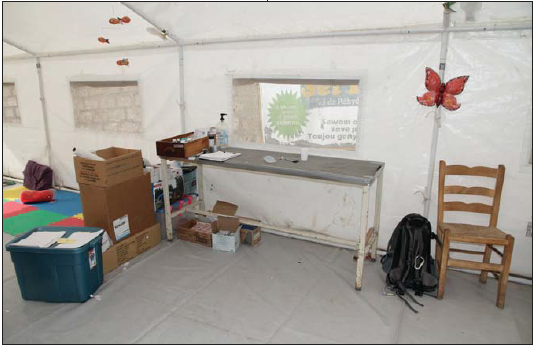
"Sterile" in Haiti is a relative term. The "sterile work field" in the tent was a single role of exam table paper, which we made last as long as possible by using just a 2-ft length for each new patient. Whenever the table (Figure 4) was really compromised with body fluids, I wiped the whole surface down with an alcohol solution. There were no paper towels, but there was plenty of toilet paper, so I used this to wipe down the table. The exam paper lasted for a week. During the second week, I was excited to find some packs of sterile surgical drape packs; we used one of the large drapes to cover each table at the start of the day, and we used the smaller drapes between patients. There were no garbage containers per se, so we scrounged cardboard boxes to put our trash in; by midday, these had attracted a lot of flies. The tent was swept at the start of each day.
 The tent was so hot that I was literally sopping wet with perspiration. I had to wipe my brow several times during each patient visit so that I didn't drip on the child when I leaned over to listen to the chest or check the ears. Each day, mopping my brow soaked through 4 cotton terry cloth towels, and I drank 3 liters of water without the need to void!
The tent was so hot that I was literally sopping wet with perspiration. I had to wipe my brow several times during each patient visit so that I didn't drip on the child when I leaned over to listen to the chest or check the ears. Each day, mopping my brow soaked through 4 cotton terry cloth towels, and I drank 3 liters of water without the need to void!
We wished more patients could have been admitted. At least 10% of the children we saw would have been admitted had we been in North America. However, there was hardly ever a bed available in the MSF pediatric tent. During the 10 days I was in Jacmel, I only admitted 3 patients: a 12-month-old baby girl with severe, likely hypertonic dehydration; a 2-year-old boy with a septic right hip; and a critically ill 12-year-old girl who was carried in on the shoulder of a relative.
 The 12-year-old's arrival brought to mind movies in which a wounded soldier, grimacing with pain, is dragged and pulled to the hopeful sanctuary of a helicopter or truck. I realized that for this girl, we were the hopeful sanctuary. She was emaciated and so weak that she could not sit. Her level of consciousness fluctuated. She had a pleural effusion on one side, a mildly and diffusely tender abdomen, and numerous shallow 0.75-cm ulcers with a green film on her labia majora. Every admission had to be approved by the MSF physician; after I described this girl's clinical situation, the experienced MSF doctor immediately replied, "She probably has HIV and TB."When I asked her how she could jump to that diagnosis so quickly, she replied, "They all have genital ulcers, and pleural effusions are common." I was advised that no anti-HIV or anti-TB medications were routinely available in Haiti.
The 12-year-old's arrival brought to mind movies in which a wounded soldier, grimacing with pain, is dragged and pulled to the hopeful sanctuary of a helicopter or truck. I realized that for this girl, we were the hopeful sanctuary. She was emaciated and so weak that she could not sit. Her level of consciousness fluctuated. She had a pleural effusion on one side, a mildly and diffusely tender abdomen, and numerous shallow 0.75-cm ulcers with a green film on her labia majora. Every admission had to be approved by the MSF physician; after I described this girl's clinical situation, the experienced MSF doctor immediately replied, "She probably has HIV and TB."When I asked her how she could jump to that diagnosis so quickly, she replied, "They all have genital ulcers, and pleural effusions are common." I was advised that no anti-HIV or anti-TB medications were routinely available in Haiti.
Whenever we had to send home children who would otherwise have qualified for admission, we asked them to come back in 1 or 2 days for follow-up and we gave them a note that allowed them to jump to the head of the line. About half of these children came back, and fortunately most were getting better.
About 60% of the children we saw were acutely ill—much like the children a pediatrician might see in a busy urban outpatient service or ER. Once our presence became known, however, we started to see more children with chronic illnesses or minor complaints—and even a few whose reason for coming might be classified as a well-child check.
In addition to the acute problem, which was usually fever or diarrhea, the children almost always had tinea, impetigo, scabies, or abdominal parasites, and often all 4 of these conditions. We gave out many topical medications for the various bacterial, insect, and fungal pathogens—and oral medications for parasites. Although I could not test for the various tropical infectious diseases, we certainly saw children whose appearance and symptoms suggested a diagnosis of malaria, dengue, or bacterial gastroenteritis. Fortunately, we had good supplies of chloroquine.
When patients needed to see a specialist . . . There were no subspecialists available to follow up on patients with seizures, nephrotic syndrome, congenital heart disease, and such. These children were given our best advice and as much medication as we could spare. For a few days, we had access to a Spanish-speaking orthopedist, and on the last Saturday, a Haitian ophthalmologist was on the premises. The ophthalmologist helped us with a 9-year-old girl with proptosis whose mother had died in the earthquake. On the day of the earthquake, the girl had been frightened and was running; she fell and hit her head. She had immediate discomfort in her right eye; by the next morning, the eye was swollen, teary, and sensitive to light, and these symptoms had persisted. The ophthalmologist suggested an ultrasound or CT scan to evaluate her for a blood clot behind the eye. Since diagnostic imaging was not available in Jacmel, I wrote a letter outlining the girl's medical situation and asked the girl's aunt to take her and my letter to the state hospital in Port-au-Prince, where we had heard that imaging and the necessary surgical intervention were available. Meanwhile, we gave her a β-blocker to help lower her intraocular pressure.
We also treated adults. Sometimes I saw adult patients who had been assessed by the physiotherapists from the TCHH rehab team. One of these was a grizzled man who looked a lot older than he was. (Actually, all the adults looked a lot older than their age; Haiti is tough on people.) This man hobbled in on crutches; he was barefoot, and the soles of his feet confirmed that he didn't wear shoes. He had a wound on top of his foot where he had been hit by a falling hammer; the therapist had asked me to check the wound. From the top, the wound looked fine, but on his sole he had a gangrenous lesion that I could have poked my gloved finger through. He had groin nodes, fever, and chills. Fortunately, the MSF team found a bed for him.
PORT-AU-PRINCE: A NICER FACILITY
The Project Medishare pediatric tent in Port-au-Prince, where I worked the last 2 days of my stay, had 40 beds, a 3-incubator neonatal ICU, a 3-bed pediatric ICU, and 2 isolation beds (I was assigned to the inpatient beds). The tent was airconditioned. The children lay on military-style cots, which were arranged side-by-side. Up to 2 family members were allowed at each patient's bedside. Thus, the 50 × 100-ft tent was very crowded and incredibly noisy. In comparison with Jacmel, however, the services were wonderful. There was a laboratory capable of processing specimens for a basic metabolic panel, urinalysis, and complete blood cell count; the lab could also handle screening tests for malaria and HIV infection. There was an x-ray machine in the tent for adults next door. The pharmacy supplies were good. Surgical support was available in the fields of orthopedics, pediatric surgery, neurosurgery, and plastic surgery. Wound care teams, physiotherapists, respiratory technicians, nurses, and psychologists were available as well.

Figure 5 – The dangerous tangle of wires shown here was a common site in Haiti— a result of the absence of an electrical code in that country; electrical burns are a frequent occurrence.
Care comparable to that in the US and Canada. All health care providers worked 12-hour shifts starting at either 7 AM or 7 PM. We examined our patients, rounded together, kept up with new problems as they arose, admitted and discharged patients, and had changeover rounds at the end of the day—not really much different from what I was used to at home. On my first day at the Project Medishare tent, I overlapped with an American team that included an internal medicine/pediatric physician, a professor of pediatrics, a fourth-year pediatric resident, and a fourth-year medical student. The care provided by this team was comparable to that seen in most pediatric hospitals in the United States and Canada.
Presenting complaints: from malnutrition to electrical burns. About one-third of the patients in the pediatric tent had either burn or trauma injuries; another third had infectious diseases; and the last third were orphans with malnutrition or other medical problems, such as idiopathic paralysis, dilated cardiomyopathy, psychosis, or cystic hygroma with airway obstruction.
Another problem we saw was electrical burns, which are commonplace in Haiti. There is no "electrical code" that ensures safe practice (Figure 5). Four children with severe electrical burns were admitted during the week before my arrival. In 2 separate incidents, power transformers "exploded" and, in each case, 2 children sustained burns on more than 75% of their skin surface. The children injured in the first incident died before my arrival, 1 of 2 adolescent sisters injured in the second incident died on my last day of work, and her sibling was not expected to survive the night. The tent was filled with the screams and the wails of the distraught mother; no one could console her. I offered her sedation, which she accepted, and eventually she cried herself to sleep.
I left Haiti with very mixed emotions. I had done my best, but my mind is filled with too many images of misery, helplessness, and poverty. Two weeks in Haiti is a long time. I'm not yet certain whether I would like to go back. If I do, next time I need to be better prepared.
For a long time to come, there will be an urgent need for health care professionals to volunteer to serve in Haiti. I definitely recommend that physicians consider giving the gift of their time and experience to help the Haitian people; I also recommend that they be physically and emotionally prepared for the experience.
