
A Rare Cutaneous Tumor
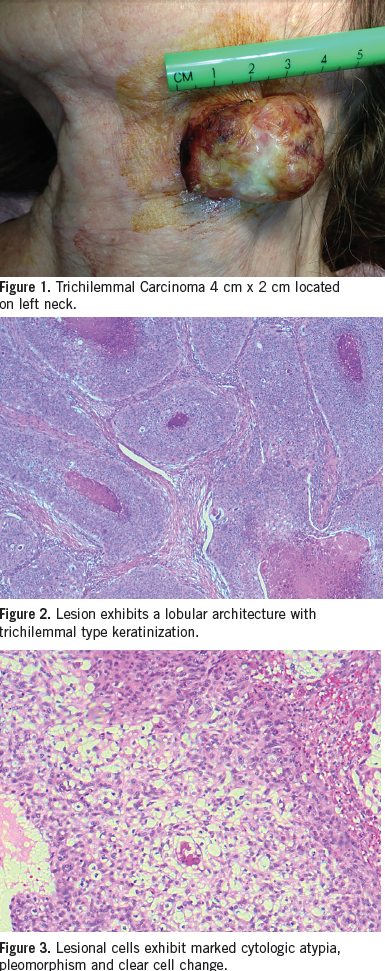 An 80-year-old white female presented to our office with a large mass on her left neck. The patient had no significant past medical history and had not been to a physician in many years. She had a history of extensive sun exposure in her younger years and did not use sunscreen protection. The mass had enlarged over a 2-year period, and had started bleeding, which prompted her to seek medical attention. The patient appeared to be otherwise healthy with no other signs of systemic illness. She was noted to have a large polypoid friable mass in her left neck that had a foul odor and was oozing blood. The lesion was approximately 4 cm by 2 cm. (Figure 1). There was no palpable lymphadenopathy.
An 80-year-old white female presented to our office with a large mass on her left neck. The patient had no significant past medical history and had not been to a physician in many years. She had a history of extensive sun exposure in her younger years and did not use sunscreen protection. The mass had enlarged over a 2-year period, and had started bleeding, which prompted her to seek medical attention. The patient appeared to be otherwise healthy with no other signs of systemic illness. She was noted to have a large polypoid friable mass in her left neck that had a foul odor and was oozing blood. The lesion was approximately 4 cm by 2 cm. (Figure 1). There was no palpable lymphadenopathy.
Laboratory results. A decision was made for immediate excisional biopsy with primary closure. The sample was sent for pathologic evaluation, which showed a large invasive tumor with overlying surface epidermal continuity, exhibiting a lobular and trabecular growth pattern with a pushing lower border. There is marked trichilemmal-type keratinization (ie, lack of granular cell layer) and the periphery of the tumor lobules show palisading (Figure 2). Focal hyaline basement membrane was identified. There was marked cytologic atypia and nuclear pleomorphism along with prominent clear cell change (Figure 3). The mitotic activity was conspicuous with rare abnormal mitoses. The clear cells show abundant periodic acid-Schiff stain positive glycogen deposition. The lesional cells were strongly positive for CK19 and epithelial membrane antigen immunostains. Focally positivity for CK 8/18 was also noted. These overall findings support the diagnosis of trichilemmal carcinoma.
Discussion. Trichilemmal carcinoma is a rare cutaneous malignancy identified by Headington in 1976. It is a malignant form of a trichilemmoma and was identified as a “histologically invasive, cytologically atypical clear cell neoplasm of adnexal keratinocytes which is in continuity with the epidermis and/or follicular epithelium.”1
Trichilemmal carcinoma is more commonly identified on the sun-exposed areas of elderly individuals with fair skin. In a literature review the age of patients varied from 9-95 with Reis et al describing the youngest patient as having xeroderma pigmentosum.2 The median age of occurrence is 71.2 Men are slightly more frequently affected than woman 1.6:1. There have been 2 cases reported in previous burn scars.3 It is usually located on the face, neck, scalp, trunk, or upper extremities. Typically these lesions appear slightly raised, pale tan or reddish, and keratotic on physical exam.
Trichilemmal carcinoma is a rare, cutaneous tumor of low- grade malignancy. Differential diagnosis includes squamous cell carcinoma, basal cell carcinoma, Keratoacanthoma, nodular malignant melanoma, epidermal cyst, and proliferative trichelemmal cysts/tumors.
Trichilemmal carcinoma is identified most commonly with histopatholigical examination of a tissue biopsy. There has been a case report of false negative diagnosis with fine needle aspiration.4
 The prognosis for these tumors is good. Most patients will respond well to a simple excision with an adequate safety margin or Mohs micgrographic surgery. There has also been a patient successfully treated with 5% topical imiquimod cream.5 A recent 2014 literature review by Hammam, et al,6 reviewed 103 reported cases treated with surgical excision. There were 35 patients with follow-up data of which 3 reported to have local recurrence and 1 had subsequent metastatic disease. They concluded that trichilemmal carcinoma is a rare neoplasm that may behave aggressively and it should be treated with complete surgical excision with histological confirmation of clear margins.7
The prognosis for these tumors is good. Most patients will respond well to a simple excision with an adequate safety margin or Mohs micgrographic surgery. There has also been a patient successfully treated with 5% topical imiquimod cream.5 A recent 2014 literature review by Hammam, et al,6 reviewed 103 reported cases treated with surgical excision. There were 35 patients with follow-up data of which 3 reported to have local recurrence and 1 had subsequent metastatic disease. They concluded that trichilemmal carcinoma is a rare neoplasm that may behave aggressively and it should be treated with complete surgical excision with histological confirmation of clear margins.7
Conclusion. The lesion was successfully treated with wide excisional biopsy and primary closure, and the patient’s outcome was excellent (Figure 4). After 2 years there has been no sign of recurrence.
References:
1. Headington JT. Tumors of the hair follicle. A review. Am J Pathol. 1976;85(2):479-514.
2. Reis JP, Tellechea O, Cunha MF, Baptista AP. Trichilemmal carcinoma: a review of eight cases. J Cutan Patol. 1993;20(1):44-9.
3. Ko T, Tada H, Hatoko M, et al. Trichilemmal carcinoma developing in a burn scar: a report of two cases. J Dermatol. 1996;23(7):463-468.
4. Allee JE, Cotsarelis G, Solky B, Cook JL. Multiply recurrent trichilemmal carcinoma with perineural invasion and cytokeratin 17 positivity. Dermatol Surg. 2003;29(8):886-889.
5. Jo JH, Ko HC, Brian Jiang HS, et al. Infiltrative tricilemmal carcinoma treated with 5% imiquimod cream. Dermatol Surg. 2005;31(8 Pt 1):973-976.
6. Hammam MS, Jiang SI. Management of trichilemmal carcinoma: an update and comphrensive review of the literature. Dermatol Surg. 2014;40(7):711-717.
7. Wilkie MD, Nazia M, Roland NJ, Lancaster J. Trichilemmal Carcinoma: a rare presentation of a cutaneous lesion. BMJ Case Rep. 2013;2013