
An Unusual Case of a Retrocardiac Mass
A 73-year-old woman who is a nursing home resident, with a past medical history of dementia and breast cancer, presented with a significant weight loss over a period of 5 months, which was associated with poor appetite. The breast cancer had been treated previously with a mastectomy (followed by a breast implant) and chemotherapy.
Laboratory, Imaging, and Biopsy Results. As part of the work-up for her weight loss and anorexia, the patient underwent a computed tomography (CT) scan of the chest. The results showed a 3.9-cm, well-defined, hyper-dense structure in the right posterior cardiophrenic angle (Figure 1). A subsequent cardiac magnetic resonance imaging (MRI) scan with gadolinium was performed, which revealed a mass density in the lower mediastinum to the right of the midline, just behind the heart (Figure 2).
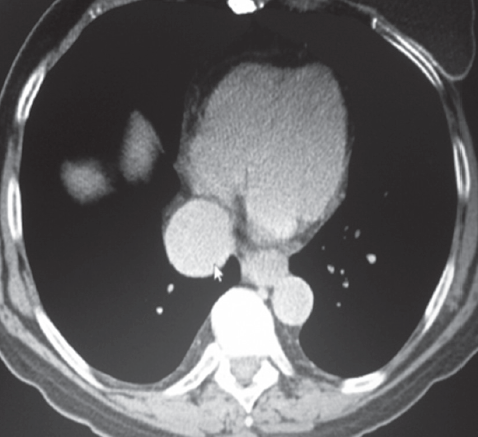
Figure 1. CT scan showing well defined hyperdense structure through the right posterior cardiophrenic angle.

Figure 2. Cardiac MRI with contrast shows mass density behind the heart with uniform enhancement by gadolinium during the venous phase.
Discussion. The chest CT scan and the cardiac MRI showed a middle mediastinal mass, which was enhanced uniformly by gadolinium during the venous phase that suggested a vascular structure. The findings were consistent with a suprahepatic aneurysm of the inferior vena cava (IVC). This is a rare condition and less than 50 cases have been reported in the world literature1-3
According to Gradman and Steinburg, IVC aneurysms are classified generally as follows:1,4,5
- Stage I: Suprahepatic IVC aneurysm without venous obstruction (as in our patient)
- Stage II: Supra or infrahepatic IVC aneurysm associated with venous obstruction
- Stage III: Infrarenal IVC aneurysm without associated venous anomaly
- Stage IV: Other
Other Associations. Middle mediastinal, retrocardiac masses are most frequently associated with the great vessels, the trachea and bronchi, the upper GI tract, and the pericardium. Though aortic aneurysms are a well-known phenomenon, their venous counterparts—ie, aneurysms of the IVC—are a rare form of middle mediastinal mass.5
Most of these IVC aneurysms are idiopathic. Some are congenital, while others are caused by trauma or arteriovenous fistulae.1 The suprahepatic variety of aneurysm is usually incidentally found on imaging as a rounded mass in the lower mediastinum,2 just behind the heart (Figure 3).
Usually patients are asymptomatic, but occasionally an aneurysm may be the site of thrombus formation. This can lead to an IVC syndrome, manifested by severe lower extremity edema, (pathogenesis being much like that of the superior vena cava syndrome of the neck and upper extremities). When the thrombus gets dislodged, pulmonary embolism can result.3,6
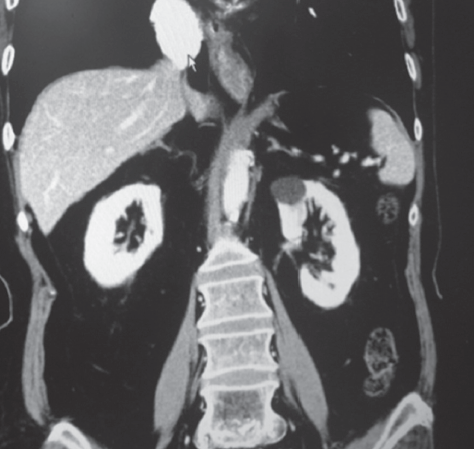
Figure 3. Coronal section on CT scan of the abdomen and lower thorax showing suprahepatic inferior vena cava (IVC) aneurysm.
Differential Diagnosis. Bronchogenic cysts are congenital cysts of tracheobronchial origin, with or without an anatomical connection with the tracheobronchial tree. They are fluid filled with fibromuscular walls. They may be located in the lower mediastinum behind the heart. Hiatus hernia would likely be in the lower mediastinum in the paracardiac or retrocardiac areas.
Pericardial cysts are congenital, thin-walled cysts, which may be round or oval and are sharply demarcated. They are most commonly located in the right cardiophrenic angle but may be seen in the retrocardiac area as well.
Tumors of the mediastinum may be primary (ie, neurogenic tumors or lymphoma) or metastatic. Depending on the cell type, they may be located in different regions of the mediastinum including the retrocardiac area.
However, none of the abovementioned 4 alternative diagnoses would demonstrate smooth and uniform pickup of intravenous contrast material on the CT scan and MRI. In this case, the diagnosis of IVC aneurysm was largely based on the location of the mass and the fact that there was uniform pickup of contrast material in the venous phase of the scans.
Outcome of the Case. In the years since the diagnosis, the patient has remained asymptomatic. She resides in a nursing home and remains quite functional.
References:
- Ensar Y, Haken G, Haldum E, et al. MDCT appearance of idiopathic saccular aneurysm of the inferior vena cava (IVC). Amer J Roentgenology. 2004;183:863-864.
- Sullivan W, Voris TK, Borlaza GS, et al. Incidental discovery of an inferior vena cava aneurysm. Ann Vasc Surg. 2002;16:513-515.
- Moustafa SE, Mookadam M, Khandheria BK, Mookadam F. Inferior vena cava aneurysm. J Am Soc Echocardiogr. 2007;20:1418e5-1418e7.
- Sullivan VV, Voris TK, Borlaza GS, et al. Incidental discovery of an inferior vena aneurysm. Ann Vasc Surg. 2002;16:513-515.
- Gradman WS, Steinburg F. Aneurysm of the inferior vena cava: case report and review of the literature. Ann Vasc Surg. 1993;7:347-353.
- Woo K, Cook P, Saeed M, Dilley R. Inferior vena cava aneurysm. Vascular. 2009;17:284-289.